A Deep Dive Into The Foundation of a Landmark Pivotal Trial and Its Long-Term Extension
Explore this page: | Study Design | Patient Characteristics
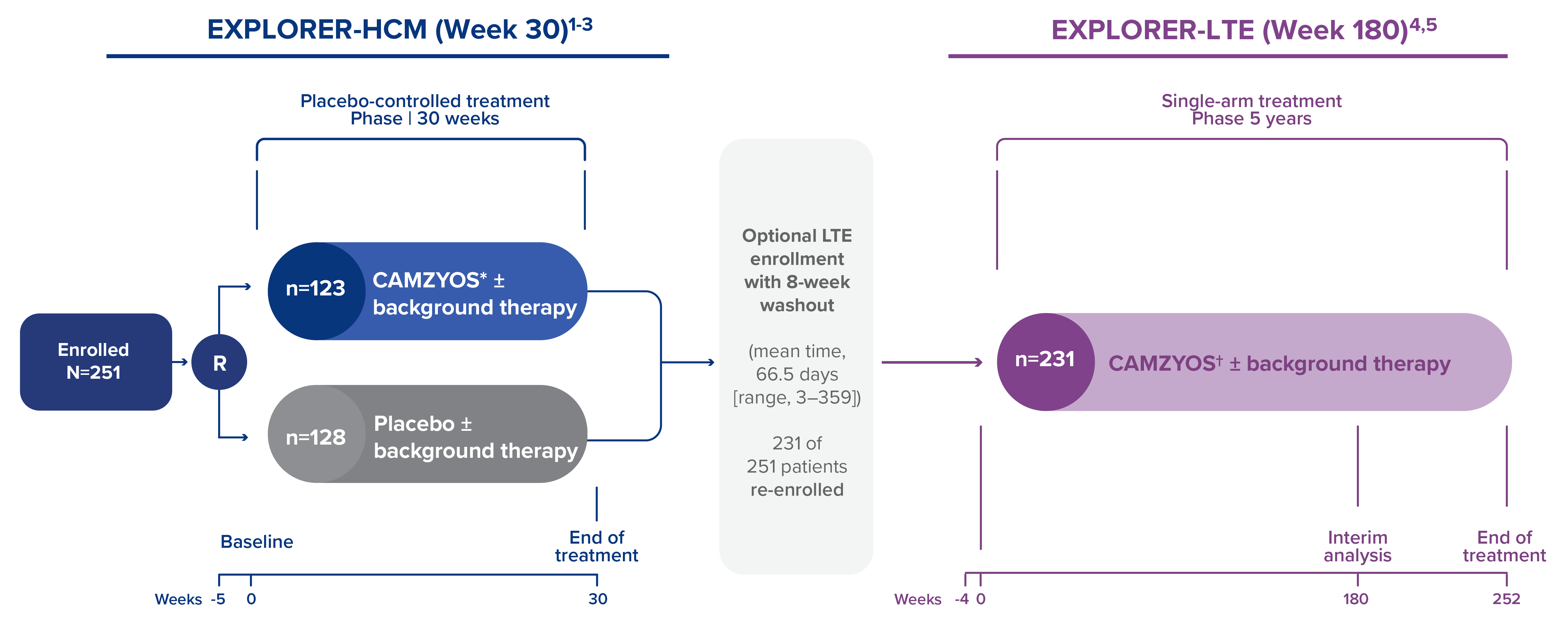
Study Design of the EXPLORER-HCM Pivotal Phase 3 Trial and Its Long-Term Extension
The majority of patients (92%) were on background therapy with a BB or CCB at baseline in both trials.2,4
EXPLORER-HCM (Week 30)
Study design2
- EXPLORER-HCM was a randomized, double-blind, placebo-controlled, 30-week, Phase 3 trial that evaluated the efficacy and safety of CAMZYOS in 251 adult patients1
Select inclusion criteria2
- Symptomatic NYHA Class ll–lll obstructive HCM
- LVOT peak gradient ≥50 mmHg and LVEF ≥55%
Select exclusion criteria1-3
- Underwent SRT within 6 months prior to screening, or planned during study
- Treatment (within 14 days of screening) or planned treatment with disopyramide, ranolazine, or a combination of BBs and CCBs
Primary composite endpoint1
- Increased exercise capacity (pVO2) and improvement or no worsening in symptoms (NYHA class)
Secondary endpoints1
|
|
Treatment1
- In the active treatment arm: 5 mg of CAMZYOS with opportunities for dose titration at Weeks 8 and 14 (based on patient response with Valsalva LVOT gradient, LVEF, and plasma concentration)
- During the treatment period, patients were evaluated every 2 to 4 weeks
EXPLORER-LTE (Week 180)4
Study design4
- EXPLORER-LTE cohort of MAVA-LTE: a single-arm, open-label, ongoing extension of the Phase 3 EXPLORER-HCM study to evaluate the long-term safety and efficacy of CAMZYOS starting at 5 mg
- 231 of 251 eligible patients from the pivotal trial enrolled in the long-term extension after an 8-week washout period
- The EXPLORER-LTE cohort of the MAVA-LTE trial sought to evaluate the long-term safety and efficacy of CAMZYOS starting at 5 mg in eligible adults who completed the EXPLORER-HCM trial. The EXPLORER-LTE cohort (n=231) is a single-arm study without an active comparator
Study objectives4
- Primary: Safety and tolerability
- Secondary: Changes in NYHA class, LVOT gradients at rest and with Valsalva, and LVEF
- Exploratory: Changes in NT-proBNP and measures of left ventricular filling
Study limitations
- These LTE data are not included in the CAMZYOS U.S. Full Prescribing Information and caution should be used in interpreting the data; there are limitations with the data including decreased sample size and different continuation rates based on the continued involvement of responders and attrition of nonresponders
- MAVA-LTE, including the EXPLORER-LTE cohort (n-231), is a single-arm study without active comparator, and data were no statistically tested for significance but are only descriptive in nature
- Patients enrolled in EXPLORER-LTE were part of either the CAMZYOS or placebo arm in the EXPLORER-HCM study; therefore, baseline characteristics for EXPLORER-LTE changed due to time and the consolidation of both arms to one cohort
In EXPLORER-HCM, all assessments for secondary endpoints were performed and Type I error was controlled in hierarchical order (sequence as indicated above) upon achieving significance in the primary endpoint (with two‑tailed P<0.05 required to proceed). Data based on all randomized patients who received ≥1 dose of study treatment. Model-estimated least-square mean differences were reported for continuous variables. Missing NYHA class data at Week 30 were imputed with the Week 26 value, in the case of NYHA response. Patients with a nonevaluable primary endpoint and NYHA secondary endpoint were considered as nonresponders. LVOT gradient, pVO2, KCCQ-23–CSS, and HCMSQ-SoB were analyzed with all available data without imputation. NYHA class was analyzed using the Cochran-Mantel-Haenszel test; continuous data were analyzed by ANCOVA (LVOT gradient, pVO2) or mixed-effect model for repeated measurements (KCCQ-23–CSS, HCMSQ-SoB).2
*5-mg starting dose was taken orally QD. The dose was periodically adjusted to optimize patient response.1 †Scheduled dose assessments of CAMZYOS in EXPLORER-LTE occurred at Weeks 4, 8, and 12 based on Valsalva LVOT gradient and LVEF, every 12 weeks through Week 156, and every 24 weeks through Week 180.2,4
BB=beta blocker; CCB=calcium channel blocker; HCM=hypertrophic cardiomyopathy; HCMSQ-SoB=Hypertrophic Cardiomyopathy Symptom Questionnaire‑Shortness-of-Breath domain score; KCCQ‑23‑CSS=Kansas City Cardiomyopathy Questionnaire (23-item version)‑Clinical Summary Score; LTE=long-term extension; LVEF=left ventricular ejection fraction; LVOT=left ventricular outflow tract; NT‑proBNP=N‑terminal pro‑B‑type natriuretic peptide; NYHA=New York Heart Association; pVO2=peak oxygen consumption; QD=once daily; R=randomization; SRT=septal reduction therapy.
Select Patient Baseline Characteristics in EXPLORER-HCM and EXPLORER-LTE1,2,4

| * | BB use at baseline derived from concomitant medication data in MAVA-LTE.4 |
| † | Nondihydropyridine CCBs.2 |
| ‡ | Data missing for one patient in the CAMZYOS group and one patient in the placebo group.2 |
BB=beta blocker; CCB=calcium channel blocker; HCM=hypertrophic cardiomyopathy; LVEF=left ventricular ejection fraction; LVOT=left ventricular outflow tract; NYHA=New York Heart Association; SD=standard deviation; SRT=septal reduction therapy.
References:
- CAMZYOS [package insert]. Princeton, NJ: Bristol-Myers Squibb Company; 2025.
- Olivotto I, Oreziak A, Barriales-Villa R, et al. Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2020;396(10253):759-769.
- Ho CY, Olivotto I, Jacoby D, et al. Study design and rationale of EXPLORER-HCM: evaluation of mavacamten in adults with symptomatic obstructive hypertrophic cardiomyopathy. Circ Heart Fail. 2020;13(6):e006853.
- Garcia-Pavia P, Oreziak A, Masri A, et al. Long-term effect of mavacamten in obstructive hypertrophic cardiomyopathy. Eur Heart J. 2024;45(47):5071-5083.
- Garcia-Pavia P, Oręziak A, Masri A, et al. Long-term effect of mavacamten in obstructive hypertrophic cardiomyopathy. Eur Heart J. 2024;45(47):5071-5083 [supplementary appendix].